Article Text

Abstract
Acute hamstring injuries are the most prevalent muscle injuries reported in sport. Despite a thorough and concentrated effort to prevent and rehabilitate hamstring injuries, injury occurrence and re-injury rates have not improved over the last three decades. This failure is most likely due to the following: (1) a lack of studies with high level of evidence into the identification and prevention of hamstring injuries and (2) a reductionist approach of the current literature. The objectives of this article are to review and critique the current literature regarding isolated risk factors, and introduce a new concept for a more comprehensive scientific understanding of how multiple risk factors contribute to hamstring strain injury. The authors hope that this new conceptual model can serve as a foundation for future evidence-based research and aid in the development of new prevention methods to decrease the high incidence of this type of injury.
Statistics from Altmetric.com
Introduction
Hamstring strains are the most prevalent muscle injuries reported in sport. Epidemiology studies have revealed that hamstring injuries alone account for between 6% and 29% of all injuries reported in Australian Rules football, rugby union, football, basketball, cricket and track sprinters.1,–,7 Frustration with hamstring strains is not only explained by the high prevalence of these injuries, but also by the prolonged duration of symptoms, poor healing responses and a high risk of re-injury rate of 12–31%.2 5 Serious concerns arise by the fact that hamstring injury and re-injury rates have not improved over the last three decades.8,–,13 In a recent epidemiologic study, Ekstrand et al10 reported injury rates over seven consecutive seasons from 23 professional European football clubs. The authors found unchanged training and competition hamstring injury rates over the 7-year period. These findings may suggest that traditional hamstring prevention and rehabilitation programmes have not been effective.
In 2003, Holm and Bahr14 elegantly highlighted, in an excellent scientific effort, the methodological weaknesses of the literature regarding hamstring injuries and proposed the criteria that should be included for identifying the influence of specific risk factors on hamstring injuries. Essentially, studies were required to be prospective with at least 200 subjects and 20–50 injuries in order to be considered minimum quality. In addition, the authors recommended multivariate statistical analysis in order to study the involvement of different risk factors.
Many prospective studies15,–,19 have been carried out after the Holm and Bahr10 article but only the studies conducted by Arnason et al,20 Gabbe et al21 and Engebretsen et al22 met the abovementioned criteria. Gabbe et al21 and Arnason et al20 reported that previous injury and age were independent risk factors for 222 Australian Football players and 305 soccer players (with a total of 31 injuries) over a full season. The authors found no association with: hip and knee flexibility, squat power, peak oxygen uptake, jump testing, body composition, adverse neural tension and so on. Engebretsen et al22 also found that previous injury was a risk factor for hamstring injury after reporting 76 injuries in 508 amateur football players. In two thorough systematic reviews, Foreman et al23 and Prior et al24 showed conflicting results and lack of consistency among the studies conducted on hamstring injuries. The authors were unable to discover a single independent risk factor for hamstring injury. They finally came to the same conclusion as Barh and Holm14 about the need for prospective studies with larger sample sizes, and including a great number of variables in order to conduct multivariate statistical analysis. Despite considerable scientific efforts, methodological quality of available research has been considered moderate (McMaster tool, mean score of 68.4%).24
The purposes of this article are to review the scientific evidence regarding risk factors for hamstring injuries, to highlight the existing limitations of the current literature and to discuss the adequacy of the current reductionist model for investigating this issue.
Risk factors for hamstring muscle strains
Previous injury
With the exception of Orchard et al,25 the literature has concluded that previous hamstring injury increases the risk of re-injury by two-to-six times.20,–,22 26,–,28 Thus, previous injury is unanimously the greatest risk factor noted. This finding prolongs the debate about whether the causes of injury are intrinsically derived from initial injury or inadequate rehabilitation. In humans, MRI has shown evidence of scar tissue for up to 1 year after an athlete's return to sport.29 The presence of scar tissue can alter muscle transmission pathway,30 decrease tendon/aponeurosis complex compliance, and consequently lead to a modification of deformation patterns in the muscle tissue adjacent to the fibrous scar. In fact, it has been recently demonstrated that previously injured muscles exhibit less tissue motion and significantly greater muscle strains near the proximal myotendinous junction compared to uninjured muscles.31 A more systematic rehabilitation programme based on objective measures and multiple risk factors would help to clarify this eternal dilemma.32
Flexibility
The literature contains controversial findings regarding the association between hamstring flexibility and the risk of injury. Seven prospective studies15 18 20,–,22 25 28 demonstrated no relationship between flexibility of the knee flexors and hamstring injury. On the other hand, three studies33,–,35 showed an association between flexibility values obtained in preseason training and the injuries suffered during the season, in studies involving professional European football players. However, the evaluation methods used to measure hamstring flexibility have been criticised for their static approach and inability to differentiate from lumbopelvic flexibility,36 which in turn has not been shown to be related to injury rates.18 21 Recently new dynamic test have been used in order to assess hamstring flexibility.33 37 Also, Dadebo et al38 observed that standard training protocols significantly reduced the rate of hamstring injuries among 30 professional English football clubs. Conversely, Arnason et al39 found no association between isolated hamstring flexibility training and a decrease in hamstring injuries in a much larger sample of Scandinavian football players. Systematic review articles from Thacker et al40 and Herbert and Gabriel41 support the findings by Arnason et al39 that stretching was not consistently associated with hamstring injuries.
An association between reduced hip flexor flexibility and the risk of hamstring injuries has been reported.42 In addition, Chumanov et al43 reported that during running, the psoas of the contralateral leg had a greater influence on hamstring length than the hamstring itself. This association should make us question the influence of adjacent joints and the use of certain measurements. Moreover, Riley et al44 have recently shown that the psoas peak elongation of the stance leg and the hamstring peak elongation of the swing leg occur at the same time during running. The assessment of analytic flexibility in a complex system should be criticised. In addition, it should be stressed that results from static measures (eg, Thomas test) should not be generalised to dynamic actions (eg, sprints).45
Strength
One of the proposed risk factors for acute hamstring injury is muscle weakness during concentric and/or eccentric contractions.5 15 16 Muscle weakness has typically been assessed with one of the following methods (1) by comparing the peak torque values of the knee extensors (during concentric contraction) with their antagonistic muscle group, that is, the knee flexors (during concentric or eccentric contraction) and (2) by comparing the peak torque values between contralateral legs during knee flexion. Both methods show conflicting findings in prospective and retrospective studies.15,–,17 25 28 46,–,49 The fact that most studies assess isokinetic strength during single-joint movements may be one of the reasons for the current controversy since the hamstrings' moment arms at the hip are nearly twice the length of those at the knee during the end of swing phase running.50 51 Sugiura et al17 recently reported that elite sprinters who sustained acute hamstring injuries had reduced concentric hip extension strength. Therefore, it may be important to assess the concentric strength of the gluteus as they help the hamstring muscles to extend the hip. More research is evidently warranted in this area.
Intervention studies aimed at reducing the incidence of hamstring injuries have focused on the use of eccentric training. In the last decade, there has been a major movement towards the use of eccentric training to treat and prevent different types of musculoskeletal disorders.39 52,–,54 However, a recent Cochrane Systematic Review conducted by Goldman and Jones55 has concluded that there is insufficient evidence to state that the protocols of eccentric training have the capacity to reduce hamstring injuries. The authors included three randomised controlled studies involving a total of 287 athletes. The study by Askling et al54 with a small sample size reported a benefit of eccentric training on hamstring muscle strains. On the other hand, Gabbe et al56 and Engebretsen et al57 found no reduction of hamstring muscle injuries after an intervention with eccentric exercises involving a greater sample size. Although one may criticise the methods employed in these studies in terms of compliance or number of subjects involved, we believe that one major limitation may be the generalised use of the Nordic hamstring exercise, which works the knee flexors eccentrically but with the hip in a fixed position. During any movement, such as the swing phase of a sprint, the hip is not fixed but instead moves and works in coordination with the rest of the segments of the body.
Core stability
Recently, core stability has been linked with hamstring injuries.43 58,–,61 Unfortunately, there are no prospective studies on the topic, but only one underpowered interventional study where Hoskins and Pollard (W Hoskins and H Pollard, unpublished data), observed a tendency towards reduced back and muscle injuries through manual therapy. There are many hypotheses that associate hamstring injuries with lumbopelvic stability.
Sherry and Best investigated the effects of two different rehabilitation programmes and found that a group of athletes who performed a core stability rehabilitation programme suffered significantly fewer hamstring re-injuries in comparison to a group of athletes that performed conventional isolated strength and stretching exercises.61 Furthermore, Chumanov et al43 have been able to demonstrate lumbopelvic influence on hamstring muscle length through the use of modelling technique. This idea is also reflected in a recent study by Kuszewski et al62 who demonstrated a tendency towards reduced hamstring stiffness following lumbopelvic stability exercises in a comparative study design. The increased stability of the abdominal muscles with concomitant liberation of the hamstrings in maintaining lumbopelvic stability may explain this phenomenon. The influence of core stability on the risk of hamstring injury requires further investigation.
Fatigue
It has been reported that there are more hamstring injuries at the end of each half of a European football game, which may suggest that fatigue acts as a risk factor for these injuries.2 10 Different fatigue protocols attempting to simulate the demands of a European football game have resulted in reductions in strength, rate of force development and muscle activity of hamstring muscles.63,–,66 However, the kinematic findings after these fatiguing protocols have produced contradictory results.67 68 While Pinniger et al67 observed a decrease in hip and knee flexion during sprinting (swing leg) after fatigue, Small et al68 revealed significant reductions in combined hip flexion and knee extension angles, indicating reduced hamstring length toward the end of each half of a multidirectional soccer-specific fatigue protocol. The different fatigue protocols may have induced different kinematic affects and may explain these contradictory findings.
Architecture
Mechanisms of hamstring injuries have been mainly studied in sprint actions, but Askling et al69,–,71 reported a series of elegant and interesting articles where different types of hamstring strains related to specific patterns of injury where studied. They reported that hamstring injuries related to sprint actions affected mainly the proximal part of the biceps femoris, whereas overstretching injuries mainly involved the free proximal portion of the semimembranosus muscle. Askling et al69,–,71 proposed anatomical and architectural reasons (fascicle length) to explain these associations. In this way, muscle functional MRI (fmMRI) has been used by our group (J Mendiguchia, unpublished data) to examine the intensity and/or pattern of muscle activation in commonly-used preventive exercises. This method relies on an exercise-induced increase on transverse relaxation times leading to recruitment images that demonstrate spatial patterns and intensity of muscle activation.72,–,76 The results suggest that different prevention exercises affect different patterns of muscle recruitment, and this degree of response differs between proximal and distal regions. These findings together with those of Askling et al69,–,71 and Kubota et al73 74 suggest that the prescribed intervention will depend on the injured muscle and its specific anatomic location.
It is well accepted that the prevalence of biceps femoris injury is much higher than the medial hamstrings.77 Thelen et al78 found that the elongation peak of the biceps femoris during sprints occurred in the oscillation phase, and to a greater magnitude, with increased speed compared to the medial hamstrings. The proximal aponeurosis of the biceps femoris is narrower than the distal part, which could explain the finding that fascicle length increases during contraction.79 Thus, the unique architecture (fascicle length, physiological cross-sectional area, aponeurosis size) of the biceps femoris may explain the greater risk of injury compared to other muscles.80 81 Considering a single muscle, it was observed with the use of complex computerised models that the greatest elongation of biceps femoris muscle fibres during an eccentric contraction takes place in the area adjacent to the proximal myotendinous junction.79 This supports the previous results shown with MRI after a hamstring strain injury in athletes.70 82 83 However, as the authors suggest, it would be desirable to confirm the findings considering all the muscles and joints in an integrated model during sprinting.79
Discussion
The purposes of this article are to review the scientific evidence regarding risk factors for hamstring injuries, to highlight the existing limitations of the current literature and to discuss the adequacy of the current model for investigating this issue. The principal finding of this review was that the scientific literature has two main flaws that may explain the unknown aetiology of these injuries. First, almost no prospective studies meet the sample (200 subjects) and incidence (20–50 injuries) criteria assessing a large number of variables that will enable multivariate statistical analysis.14 Second, and perhaps more important, the limitations inherent to the current reductionist model used to study hamstring injuries.
Research has traditionally assumed a reductionistic view84 where a linear and unidirectional causal-effect model was systematically followed in many topics. This reductionist model is clearly influenced by the Western understanding of any phenomenon and conceives any system as the sum of its parts (figure 1). The medical understanding of the human body as an entity assembled from many pieces stems from Aristotle's premises, showing the ancestral origin of this still current reductionist model. These parts are studied analytically in order to define the contribution of each one into the whole. Currently, there is no clear explanation or robust model that consistently demonstrates how all of the risk factors interact because a reductionistic model does not consider the inter-relationships and random mixing of the parts.84 As an example, can impaired flexibility be considered as a risk factor for hamstring injury as suggested by different prospective studies? If we isolate flexibility of the knee flexors in a hamstring injury study, we may skip the influence of core muscles43 and many other parameters like adverse neural tension85 on flexibility itself.
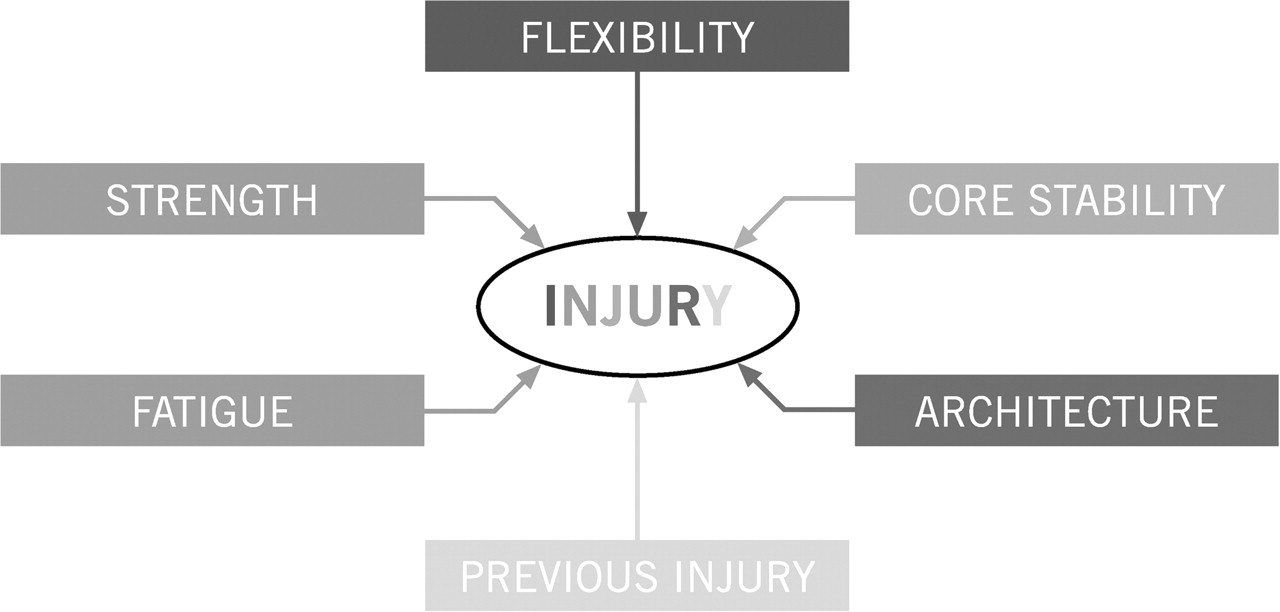
Current cause – effect model for hamstring strain injury.
This analytical approach, allows correlational and regression analysis. Both may be useful when developing a research question, but the knowledge they provide may be too limited.84
With these caveats in mind, one must try to consider a less reductionistic model in which the whole body is involved, assuming that parts are not homogeneous and that intimate relationships are present in a non-random fashion.84 This new conceptual model would assume an interconnected, multidirectional and synergic interaction between all parts (figure 2). With this model, many assumptions about hamstring injuries may be cleared. For example, Franz et al45 have recently shown that an excessive contraction of the hip flexors may cause an anterior pelvic rotation, compensated with a lumbar hyperlordosis, resulting in a lack of hip extension. In fact, pelvic anteversion has been associated with a decrease in the activity of the gluteus muscles.86 It might be speculated that these findings could help to explain the results obtained by Brughelli et al,87 where injured subjects showed reduced horizontal but not vertical strength (ie, during running) due to a likely hip extension range-of–motion (ROM) deficit. The take-to-home message of this example is that one should compare mobility with strength variables without the need to isolate them, thus achieving a more global approach and understanding.

{kind=link}
{kind=link}
New conceptual model for hamstring strain injury.
New ‘in sim’ methodological approach enables forward dynamic simulations and the possibility to modify different parameters.84 88 This may help to explain how lumbopelvic stability affects hamstring flexibility and strength, and even muscle fibre length, and confirms the suspicions mentioned by different authors.61 62 Thus, research should approach inter-relationships between multiple variables, for example, ‘core’ stability, muscle flexibility, strength and/or muscle architecture should be advocated to be a more complex model in which hamstring injuries are based.
This new conceptual model may be applied to give light to the hypothesis that a decreased activation and/or strength of the gluteus muscles may explain an increased activation of the hamstring muscles, leading to an increased risk of injury. This hypothesis has been recently supported by a case report by Wagner et al.89 The model may be even used to investigate the optimum percentage of strength for hamstring muscles to maintain pelvic stability90,–,92 and extend the hip and flex the knee at the same time.
In another example, McHugh et al85 and Méndez-Sánchez et al93 recently verified the effect of adverse neural tension on ROM. Neural tension has not been shown to be a risk factor24 but it may indirectly have an affect through decreased ROM. But do we know which effects both have on the capacity to produce strength? This example shows how a variable that is not considered a risk factor, may turn into a risk factor when combined with others, and increase the likelihood of injury.
With these examples and the pattern shown in figure 2, we obtain a more realistic picture of what actually occurs during injury, and we move away from the reductionist vision and design that prevails in the current literature.
Although beyond the scope of analysis of this manuscript, we have not to forget the role that external factors, behaviour,94 95 environment95 and genetics may play in hamstring injuries. It is likely that an adequate understanding of these factors may lead to improvements in the prevention of hamstring injuries in sport.
What is already known on this topic
▶ Hamstring injury and re-injury rates have not improved over the last three decades.
▶ Current research methods based in unidirectional and analytical approaches neglect the multifactorial condition and complexity of hamstring injuries.
What this study adds
A new conceptual model showing inter-relationship between the different factors involved in hamstring strains can provide a better understanding of this multifactorial injury and therefore improve its prevention and prediction methods.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.